This article was published in partnership with The Marshall Project, a nonprofit news organization covering the US criminal justice system, Reveal, and USA Today. Sign up for The Marshall Project’s newsletters, and follow them on Instagram, TikTok, Reddit, and Facebook.
Susan Horton had been a stay-at-home mom for almost 20 years, and now—pregnant with her fifth child—she felt a hard-won confidence in herself as a mother.
Then she ate a salad from Costco.
It was her final meal before going to Kaiser Permanente hospital in Santa Rosa, in Northern California, to give birth in August 2022. It had been an exhausting pregnancy. Her family had just moved houses, and Horton was still breastfeeding her toddler. Because of her teenage son’s heart condition, she remained wary of Covid-19 and avoided crowded places, even doctor’s offices. Now, already experiencing the clawing pangs of contractions, she pulled out a frozen pizza and a salad with creamy everything dressing, savoring the hush that fell over the house, the satisfying crunch of the poppy seeds as she ate.
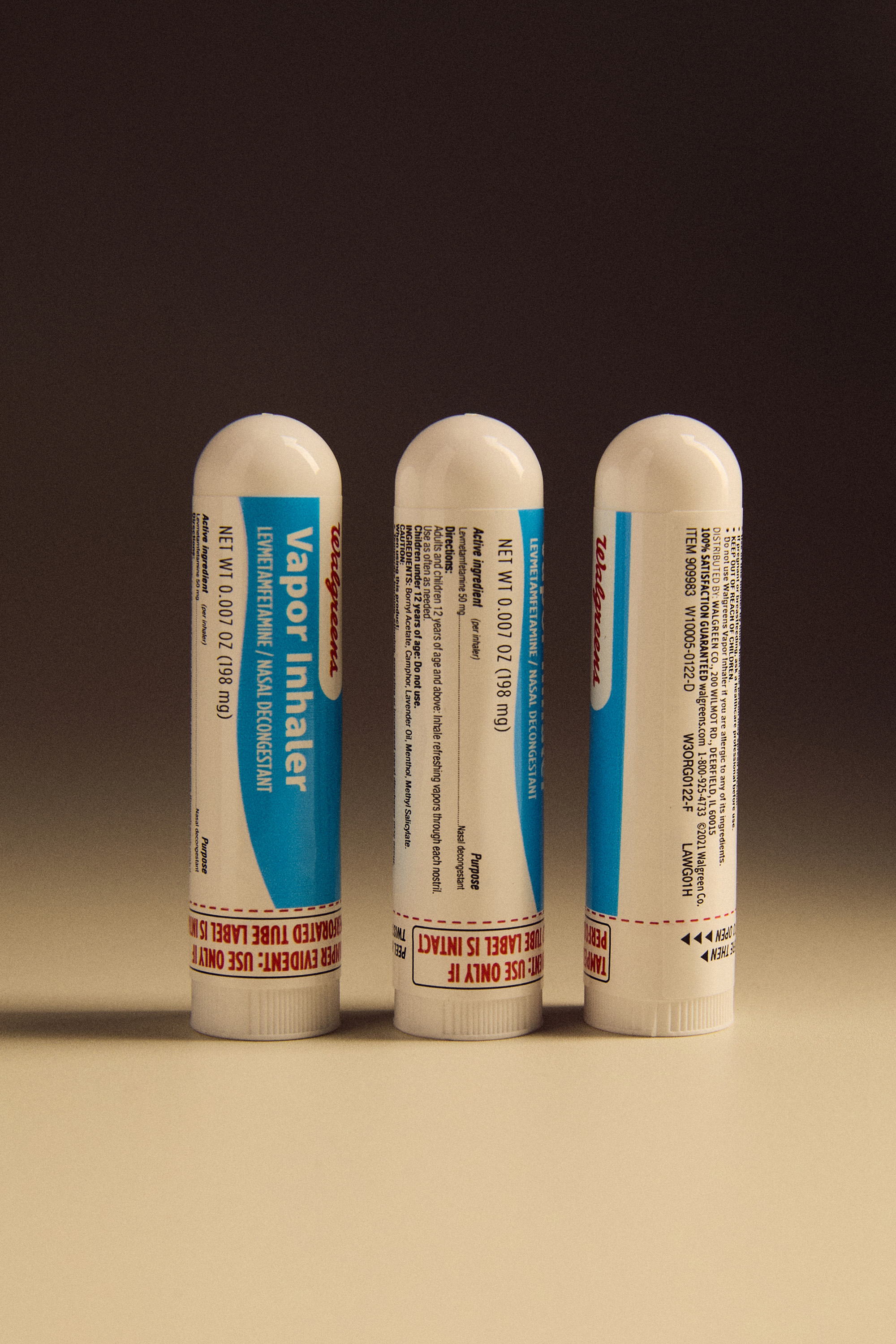
Horton didn’t realize that she would be drug-tested before her child’s birth. Or that the poppy seeds in her salad could trigger a positive result on a urine drug screen, the quick test that hospitals often use to check pregnant patients for illicit drugs. Many common foods and medications—from antacids to blood pressure and cold medicines—can prompt erroneous results.
The morning after Horton delivered her daughter, a nurse told her she had tested positive for opiates. Horton was shocked. She hadn’t requested an epidural or any narcotic pain medication during labor—she didn’t even like taking Advil. “You’re sure it was mine?” she asked the nurse.
If Horton had been tested under different circumstances—for example, if she was a government employee and required to be tested as part of her job—she would have been entitled to a more advanced test and to a review from a specially trained doctor to confirm the initial result.
But as a mother giving birth, Horton had no such protections. The hospital quickly reported her to child welfare, and the next day, a social worker arrived to take baby Halle into protective custody.


Kaiser Permanente declined to comment on Horton’s care. A spokesperson said the Santa Rosa hospital typically gets consent to drug-test patients for medical reasons, and as a mandated reporter under state law, it refers potential exposures of newborns to illicit drugs to child welfare authorities.
The Sonoma County Human Services Department said, in a statement, that it evaluates all referrals using “evidence- and research-based” methods, and if a report is deemed valid, it has a duty under state law to investigate.
Horton said the experience made her feel powerless and terrified.
“They had a singular piece of evidence that I had taken something,” she said, “and it was wrong.”
For decades, state and federal laws have required hospitals across the country to identify newborns affected by drugs in the womb and to refer such cases to child protective services for possible investigation. To comply, hospitals often use urine drug screens that are inexpensive (as little as $10 per test), simple to administer (the patient pees in a cup), and provide results within minutes.
But urine drug screens are easily misinterpreted and often wrong, with false positive rates as high as 50 percent, according to some studies. Without confirmation testing and additional review, false positive results can lead hospitals to wrongly accuse parents of illicit drug use and report babies to child welfare agencies—which may separate newborns from their families, an investigation by The Marshall Project and Reveal has found.
It’s unclear how many of the nation’s 3.6 million births every year involve drug testing, but health care experts said urine screening is ubiquitous. Tens of thousands of infants are reported annually to authorities for in utero drug exposure, with no guarantee that the underlying tests are accurate, our analysis of federal data shows.
“They had a singular piece of evidence that I had taken something, and it was wrong.”
To report this story, The Marshall Project interviewed dozens of patients, medical providers, toxicologists, and other experts, and collected information on more than 50 mothers in 22 states who faced reports and investigations over positive drug tests that were likely wrong. We also pored over thousands of pages of policy documents from every state child welfare agency in the country.
Problems with drug screens are well known, especially in workplace testing. But there’s been little investigation of how easily false positives can occur inside labor and delivery units, and how quickly families can get trapped inside a system of surveillance and punishment.
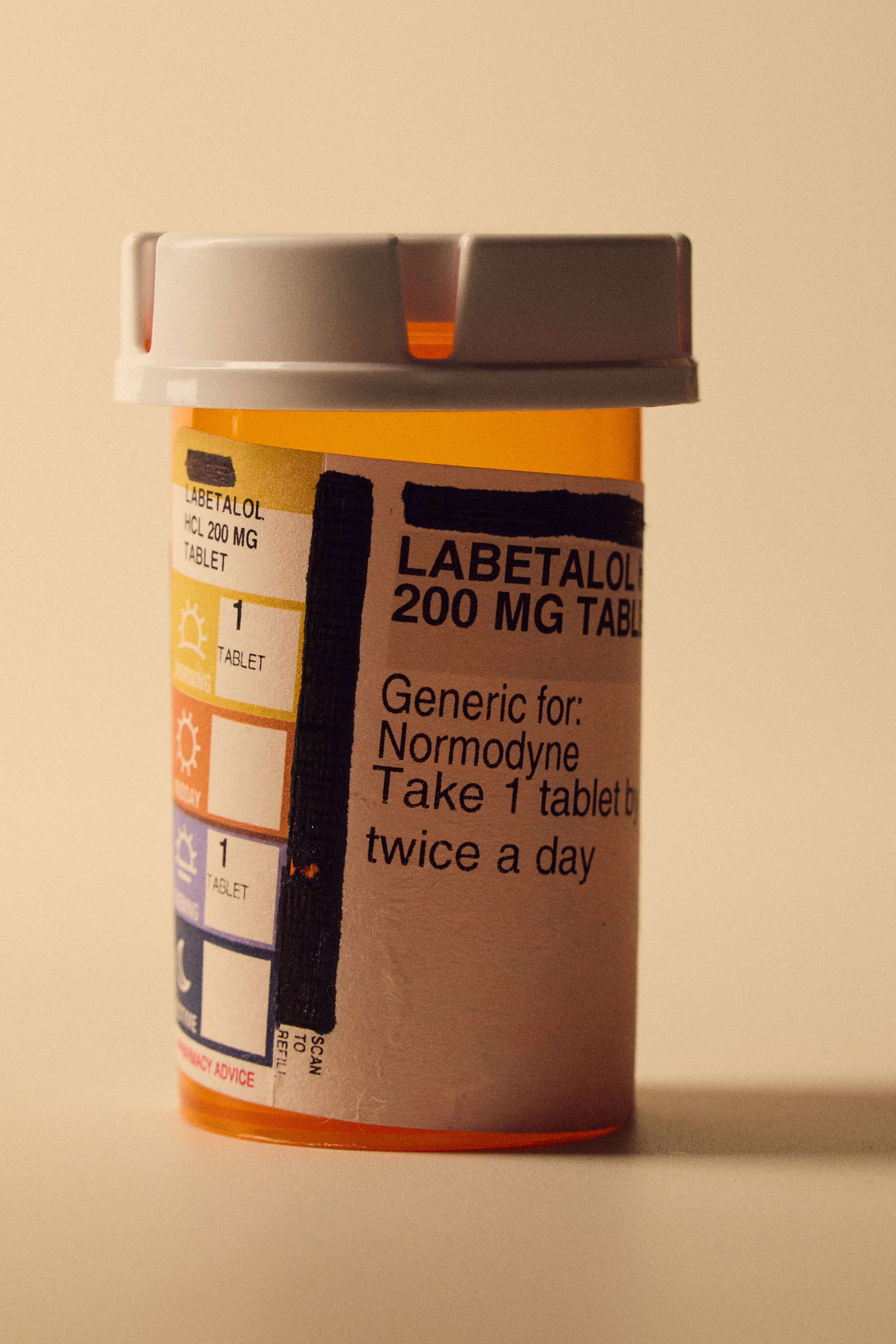
Hospitals reported women for positive drug tests after they ate everything bagels and lemon poppy seed muffins, or used medications including the acid reducer Zantac, the antidepressant Zoloft, and labetalol, one of the most commonly prescribed blood pressure treatments for pregnant women.
After a California mother had a false positive for meth and PCP, authorities took her newborn, then dispatched two sheriff’s deputies to also remove her toddler from her custody, court records show. In New York, hospital administrators refused to retract a child welfare report based on a false positive result, and instead offered the mother counseling for her trauma, according to a recording of the conversation. And when a Pennsylvania woman tested positive for opioids after eating pasta salad, the hearing officer in her case yelled at her to “buck up, get a backbone, and stop crying,” court records show. It took three months to get her newborn back from foster care.
Federal officials have known for decades that urine screens are not reliable. Poppy seeds—which come from the same plant used to make heroin—are so notorious for causing positives for opiates that last year the Department of Defense directed service members to stop eating them. At hospitals, test results often come with warnings about false positives and direct clinicians to confirm the findings with more definitive tests.
Yet state policies and many hospitals tend to treat drug screens as unassailable evidence of illicit use, The Marshall Project found. Hospitals across the country routinely report cases to authorities without ordering confirmation tests or waiting to receive the results.

At least 27 states explicitly require hospitals to alert child welfare agencies after a positive screen or potential exposure, according to a review of state laws and policies by The Marshall Project. But, not a single state requires hospitals to confirm test results before reporting them. At least 25 states do not require child welfare workers to confirm positive test results, either.
While parents often lack protections, most of the caseworkers who investigate them are entitled to confirmation testing and a review if they test positive for drugs on the job, our analysis found.
Health care providers say there are medical reasons to test labor and delivery patients for drugs, including alerting doctors to watch a newborn for withdrawal symptoms. They also cite concerns about criminal and legal liability if they fail to report positive test results.
Even when a doctor refutes a positive result and vouches for their patient, hospitals may report the incorrect data anyway to child welfare agencies.
“It’s almost like a gut punch. You come to the hospital and you see a social work note on your patient’s chart,” said Dr. Yashica Robinson, an OB/GYN in Huntsville, Alabama, who has tried and failed several times to halt child welfare reports and investigations of patients with false positive results. “Once that ball is rolling, it’s hard to stop it,” Robinson said.

No government agency collects comprehensive data on false positive results or on how many pregnant patients are tested. And confidentiality laws that shield medical and child welfare records make it difficult for the public to understand how many families are affected.
In 2016, Congress mandated states to submit the number of “substance-affected” infants to the U.S. Department of Health and Human Services. Not all states track every case, but from fiscal years 2018 through 2022, medical professionals reported at least 170,000 infants to child welfare agencies for exposure to substances, according to an analysis by The Marshall Project. In 2022 alone, more than 35,000 such cases were reported, and authorities removed more than 6,000 infants from their families, our analysis found.
The harms of drug testing fall disproportionately on low-income, Black, Hispanic, and Native American women, who studies have found are more likely to be tested when they give birth, more likely to be investigated, and less likely to reunite with their children after they’ve been removed.
But the false positive cases The Marshall Project identified include parents of all socioeconomic classes and occupations—from a lawyer to a school librarian to a nurse who drug-tests other people for a living.
“People should be concerned,” said Dr. Stephen Patrick, a leading neonatal researcher who chairs the Department of Health Policy and Management at the Rollins School of Public Health in Atlanta. “This could happen to any one of us.”
“People should be concerned. This could happen to any one of us.”
Drug screens are more guesswork than exact science. Chemicals in the tests quickly cross-react with urine, flagging anything that looks like it could be an illicit substance. The tests are like fishing nets that are cast wide and pick up anything and everything that fits, said Dr. Gwen McMillin, a professor at the University of Utah School of Medicine and medical director of a drug-testing lab. The problem is that nets also ensnare fish that aren’t being targeted: compounds that are closely related to illicit substances or merely look similar.
“Drug testing results need to be confirmed before they go to CPS,” McMillin said. “Actions should not be taken based on a single drug testing result. Period.”
But sometimes, even confirmation tests can be misinterpreted, as Susan Horton found. At first, Horton was puzzled by her positive test result. She wondered if her urine might have been mixed up with another patient’s. Then—“ding ding ding!”—her last meal popped into her head. She told a nurse about the poppy seeds in her salad, sure that this would resolve her doctors’ concerns.


Horton’s records show Kaiser ran her urine sample through a second test, and this time it came back positive for one opiate in particular: codeine. That shouldn’t have been surprising—poppy seeds, like the ones in Horton’s salad, are derived from the opium poppy plant and contain codeine.
To differentiate between salad dressing or bagels and illicit drugs, toxicologists have long recommended testing urine for the presence of a compound called thebaine, which is found in poppy seeds but not in heroin. There’s no indication that the hospital performed or even knew about the thebaine test, leaving providers with no way to prove or disprove Horton’s claims.
“Mom and dad insistent that a Costco salad with poppyseed dressing is responsible,” a doctor wrote in her notes. Another doctor wrote: “We are unable to verify whether this could result in a positive test.”
Soon, multiple doctors and nurses filed into Horton’s room. They said hospital policy dictated that Halle remain there for five days to be monitored for possible drug withdrawal symptoms—“for baby’s safety,” a doctor told Horton.
Unlike most other states that require hospitals to report positive drug tests, California law says a positive test alone “is not in and of itself a sufficient basis for reporting child abuse or neglect.” But because of Covid-19 and her son’s heart condition, Horton had also missed some prenatal appointments, which many providers see as a red flag for drug use. A hospital social worker noted the missed appointments and decided to file a report.
In a statement about its practices in general, Kaiser said it always conducts a “multi-faceted assessment” prior to filing a report to CPS, which is responsible for reviewing the information and investigating.
Horton insisted that keeping her baby at the hospital was unnecessary. “I’m not a drug addict,” she said she pleaded. Desperate for help, her husband called the police, who declined to oppose hospital directives, records show.

When the caseworker arrived, the couple refused to sign a safety plan or allow the person to interview their children and inspect their home. So the caseworker immediately obtained a judge’s order and placed baby Halle into temporary custody in the hospital, before discharging her to her grandparents, who were ordered to supervise Horton with her child.
A few days later, Horton stood silently in court, dressed in pants that clung uncomfortably to her still-healing body, feeling as if her motherhood was on trial. A caseworker told the judge it would be dangerous to release Halle to her parents, and Horton agreed to another drug test. A worker followed her to the bathroom and watched her urinate in a cup.
By then, caseworkers and doctors had privately acknowledged that poppy seeds could have caused Horton’s positive test result. But in court the caseworker didn’t mention that. Instead, she argued that Horton’s purported drug use had “caused serious physical harm” to her child.
The agency said under state law it can’t comment on individual cases. Speaking generally, it said a single positive drug test, false or otherwise, doesn’t warrant an investigation, and that there needs to be “a reported observation of impact to the child.”
When workplace drug testing was introduced in the 1980s, unions and civil rights groups decried the error rates of drug screens and how companies were firing workers over false positive results. In response, federal authorities mandated safeguards for employees, including requiring confirmation tests and a review from a specially trained doctor to determine whether a food or medication could have caused a positive result.
A federal medical advisory committee in 1993 urged health care providers who drug-test pregnant patients to adopt the same rigorous standards. But amid the “crack baby” panic, the idea of protecting mothers did not catch on.
Hospital drug testing policies vary widely. Many facilities, such as Kaiser in Santa Rosa, test every labor-and-delivery patient. Other hospitals flag only certain people, such as those with limited prenatal care, high blood pressure, even bad teeth, experts say. At many hospitals, the decision is up to doctors and nurses, who may view a mother’s tattoos, disheveled clothing, or stressed demeanor with suspicion. Studies have found that the decision to test is rife with class and race bias.
“Those who look like they have less resources, people might say, ‘Well, they look more likely to use drugs,’” said Dr. Cresta Jones, an associate professor and maternal-fetal medicine specialist at the University of Minnesota Medical School.
Hospitals often have full discretion over whether to screen for drugs, but once a positive result is in hand, the decision to report becomes more complicated. Laws and policies in at least 12 states explicitly require hospitals to send screen results to child welfare agencies, even if they are not confirmed, according to The Marshall Project’s review.

For hospitals, cost is also an issue. While urine screens are cheap, the equipment needed to run a confirmation test costs hundreds of thousands of dollars, in addition to the cost of expert personnel and lab certification. Some hospitals contract out confirmation testing—a lower-cost alternative—but getting results can take days, long after many families are ready to go home.
Doctors, nurses, and hospital social workers face an uncomfortable predicament: Do they send the baby home to what they believe could be an unsafe environment, or do they call authorities?
“God forbid the baby goes home, withdraws and dies, we’re going to be held liable for that,” said Dr. Adi Davidov, an obstetrician at Staten Island University Hospital, which drug-tests every birthing patient.
State mandatory reporting laws add to the pressure on doctors and nurses. These laws impose criminal liability on providers who fail to report, while also protecting physicians who report “in good faith”—insulating hospitals from lawsuits if test results are wrong.
Even when doctors have the ability to order a confirmation test, they don’t always do so. Many misinterpret positive screens as definitive evidence of drug use.
“We were guilty until proven innocent.”
When Grace Smith had her fourth child in 2021 at St. Luke’s University Hospital, an hour north of Philadelphia, she was taking prescribed marijuana and Vyvanse, a medication for attention deficit hyperactivity disorder. The medicine contains amphetamine, but the hospital’s drug screen results did not differentiate between meth and amphetamine, according to medical records. The day after Smith delivered her son, a doctor told her that she and her baby had tested positive for meth and that the hospital had notified child protective services.
Smith’s husband, Michael, asked the doctor to review his wife’s medical records to confirm her prescription, according to the doctor’s notes. The doctor argued that wasn’t her role. “I explained that our responsibility as healthcare workers was to report the case” to child welfare authorities, she wrote, adding that the agency “would conduct any investigation that was necessary.”
When Michael Smith told the doctor they were leaving with their baby, the hospital called the police. An officer escorted the parents out, without their newborn, a police report shows. The Smiths said the police told them they would be arrested if they returned.
A spokesperson for St. Luke’s University Health Network declined to answer questions from The Marshall Project, saying in an email that the hospital “complies with all rules and regulations regarding drug testing and reporting” and that the newborn’s welfare “is always our primary concern.”
Four days after the Smiths’ son was born, Monroe County Children and Youth Services told the hospital it was okay to release the baby to his parents. But the investigation remained open. It wasn’t until the Smiths paid more than $3,500 for a lawyer—and nearly $300 for a confirmation drug test that came back negative—that the agency closed their case. The agency declined to comment.
The Smiths filed a lawsuit in 2022 against St. Luke’s. In its response, the hospital acknowledged that it had not given Grace a confirmation test, but denied violating the Smiths’ privacy or civil rights. A judge dismissed the suit in 2023, saying in part that the Smiths did not sufficiently argue their claims.

Many providers erroneously assume that child welfare agencies verify a parent’s drug use. But government caseworkers typically lack the expertise to accurately interpret drug test results. State policy manuals seldom mention the possibility of false positives. It often falls on parents to prove their own innocence.
As a nurse in South Carolina, Ashley Riley said she regularly drug-tested patients in an addiction treatment program, flagged faulty tests, and sent out positive screens for confirmation. But when she herself screened positive for opiates after delivering her son in 2023, Riley said the hospital declined to order a confirmation test, then reported her to authorities.
Riley and her husband, Jeffrey, insisted the positive result was from lemon poppy seed muffins that she had eaten throughout her pregnancy. As proof, Jeffrey Riley texted the investigator a receipt for the muffins, studies on false positives caused by poppy seeds, and the 2023 memo from the Department of Defense urging service members to avoid poppy seeds.
“At no point in time was there anybody in there that was even trying to advocate for my wife, except for me,” he recalled.
At first, he thought his efforts were working. The caseworker acknowledged in his notes having seen the poppy seeds and noted that the report “could be falsified.”
But the caseworker still insisted the couple sign a safety plan, advising them that their two children would be placed in foster care unless they assigned a “protector”—a responsible adult who would supervise them with their children at all times. This continued for 45 days before the case was closed as unfounded.
“We were guilty until proven innocent,” Ashley Riley said.
The hospital even charged $424 for the problematic urine test. Hospital officials did not respond to multiple interview requests.
Will Batchelor, a spokesperson for the South Carolina Department of Social Services, wrote in a statement that the agency has a duty to investigate once a hospital has filed a report and that it “exercised appropriate restraint” by not removing the child from the home.
“Because the safety of a child is at stake, DSS has to continue its investigation beyond seeing a receipt for poppy seed muffins,” Batchelor wrote.
Even when a parent has a confirmation test and her own doctor’s word attesting to a false positive result, authorities may keep investigating.
When Melissa Robinson, an elementary school librarian in Huntsville, Alabama, screened positive for cocaine in early 2024, the news shocked her and her doctors. Robinson had avoided anything during her pregnancy that could be risky, even cold cuts—which may carry bacteria—and had no history of drug use. Because of the positive test, staff told Robinson she was not allowed to breastfeed her daughter, hospital records show, and they reported her to Alabama’s child welfare agency, the Department of Human Resources. Robinson said a caseworker told her that she probably wouldn’t be allowed to be alone with her baby—her husband would have to supervise.
A few days later, a confirmation test came back negative for any substances. With proof that she had not used cocaine, Robinson assumed the case would be closed. Instead, the agency continued to investigate, inspecting her home and even requiring her husband to take a drug test, she said.

A spokesperson for Alabama’s child welfare agency said they are required to respond immediately to a hospital report and “make safety decisions relying on current and most accessible information.”
When the baby was two weeks old, the agency closed the case, citing insufficient evidence. But the allegations will remain on Robinson’s record for at least five years.
“To have such a beautiful experience tainted by something like that, it’s difficult,” Robinson recalled. “Truthfully, it’s turned me into somebody different.”
“To have such a beautiful experience tainted by something like that, it’s difficult. Truthfully, it’s turned me into somebody different.”
Some medical groups and providers have taken steps to reduce unnecessary child welfare reports. The American College of Obstetricians and Gynecologists advises hospitals to use a screening questionnaire rather than drug tests to identify people who may have substance abuse problems. The organization also recommends that hospitals obtain consent from patients, explaining the potential consequences of a positive result—including if the hospital is required to report it to authorities. A number of large hospitals have adopted some version of those recommendations.
After a study at Staten Island University Hospital in New York found a high rate of false positives, administrators brought the confirmation testing in-house. They said results come back within a day or two, rather than the week that is typical for outside tests, which allows providers to wait before contacting child welfare.
“Any time you act on a test that’s not 100 percent, you run the risk of causing more harm than good,” said the hospital’s Dr. Davidov. “If you are going to get CPS involved with a mother who did nothing wrong and is a good citizen, that’s harming her. It’s harming her experience, it’s harming her ability to take care of her newborn.”
In recent years, advocacy groups have filed lawsuits against hospitals for testing without explicit consent, which has led some state officials and lawmakers to speak out against the testing. But in most of the United States, it remains common practice to report families based on unconfirmed positive screens. Most of the women interviewed by The Marshall Project signed general consent forms at the hospital but said they were never informed explicitly they would be drug-tested, nor that a positive result could be reported to authorities.

For Susan Horton, her family’s ordeal has created an undercurrent of fear that courses through her daily life.
After the court hearing in August 2022, child welfare workers took the baby to Horton’s elderly in-laws and barred Horton and her husband from being alone with their newborn while the agency investigated. Finally, almost two weeks after their daughter was born, the agency withdrew its petition and a judge dismissed the case, allowing the Hortons to bring baby Halle home.
One afternoon last spring, Horton took her daughter, now a toddler, outside. Halle giggled as her mother chased her around the front yard, her little feet splashing in a small mud hole. This was the life Horton had envisioned years ago—a quiet place in the California countryside where her children could delight in the world around them. And yet, Horton couldn’t help but remember the investigation that destroyed her family’s peace of mind—and her self-esteem.
“I had a lot of confidence in how I mother and how I parent,” she said. “Now in my head, I’m always questioning my choices.” She wondered aloud what neighbors would say if they saw her daughter playing in the mud, if someone might accuse her of being a bad parent.
“I just always have that looming feeling that at any moment CPS could come knocking and take my children away.”
Marshall Project reporters Weihua Li, Andrew Rodriguez Calderón, Nakylah Carter, and Catherine Odom contributed to this story.